Before the Emergency: Why Neuroinclusive Design Belongs in Emergency Planning

Emergency planning is not only about having an exit. It is about whether people can find, understand, and trust the route under stress.
Ahead of AIANY Social Science and Architecture’s upcoming event, “People and Buildings Under Stress: Neuro-Inclusive Design and Emergency Planning,” I have been thinking about what changes when architects enter the emergency planning conversation.
It is a more important shift than it may appear at first.
Emergency planning is often treated as an operations issue. A compliance issue. A facilities issue. A safety protocol. A binder on a shelf. A checklist that gets reviewed, filed, and occasionally rehearsed.
All of that matters.
But emergency planning is also a design issue.
Because the built environment does not just contain an emergency response. It shapes it.
A building shapes whether people can receive information, understand what to do, find a safe route, tolerate a crowd, wait safely, regulate stress, and interact safely with staff or first responders.
That is especially true for neurodivergent people, people with heightened sensory sensitivities, people with cognitive or communication needs, older adults, disabled people, children, and anyone whose ability to process information changes under pressure.
And under emergency conditions, that can include almost everyone.
Emergency Plans Often Assume a Narrow User Model
As we wrote recently in Emergency Response Was Never Designed for Neurodivergence, emergency systems are often built around assumptions of speed, clarity, control, and predictable behavior. The challenge is that real people do not always experience emergencies that way.
They assume people can stay calm. They assume people can process instructions quickly. They assume people can tolerate alarms, flashing lights, crowding, uncertainty, and sudden changes in direction. They assume people can move predictably, follow directions immediately, and make fast decisions while under stress.
But real emergencies do not happen to an idealized user.
They happen to real people.
A person may freeze. They may shut down. They may panic. They may move slowly. They may become disoriented. They may miss auditory instructions. They may struggle to read signage. They may need more time, more context, less noise, or a quieter place to wait.
A person’s behavior may also be misread. A delayed response, lack of eye contact, inability to move, or visible distress can be interpreted as noncompliance when it is actually overload.
People do not fail emergency systems. Emergency systems fail people when they assume everyone responds the same way under stress.
This is one of the central questions behind neuroinclusive emergency planning: What happens when the plan meets the real conditions of the human body and mind under pressure?
Emergency Conditions Are a Crash Test for Emergency Plans
Emergency conditions are a crash test for emergency plans.
A plan that works on paper may not work for real people under sensory, cognitive, and emotional stress. The real test is not whether a plan exists. The real test is whether it performs when people are scared, overloaded, confused, separated from support, navigating unfamiliar space, or relying on staff who are also under pressure.
That is why this conversation belongs in architecture and design.
Buildings are not passive during emergencies. They communicate. They direct. They confuse. They calm. They amplify stress. They create bottlenecks. They offer refuge. They shape decisions.
When we look at emergency planning through a neuroinclusive design lens, we begin to ask better questions.
Can people understand the alert?
Can they tell where to go?
Is the safest route also the most legible route?
What happens when alarms, lights, and crowds create sensory overload?
Where can someone pause without blocking movement or appearing suspicious?
Can staff recognize distress without escalating conflict?
Does the plan account for people who need more time, different communication, or lower-stimulation space?
These are not abstract questions. They are practical safety questions.
Four Dimensions of Emergency Response in the Built Environment
Neuroinclusive emergency planning asks how communication, movement, sheltering, and response perform for real people under stress.
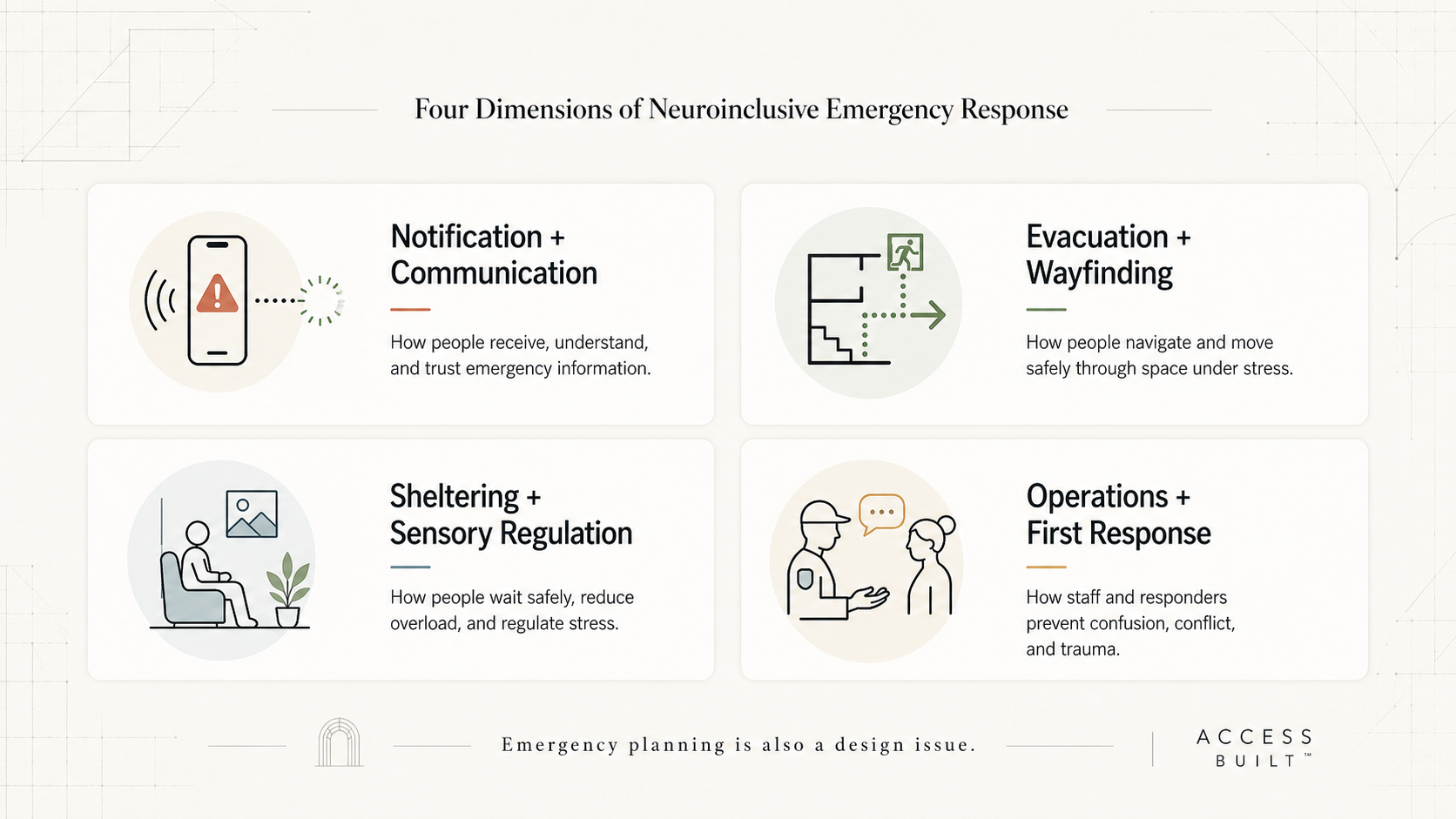
The AIANY event focuses on four critical dimensions of emergency response: notification and communication; evacuation, navigation, and wayfinding; sheltering in place; and operations and first response.
Each of these areas is operational. But each is also spatial, sensory, behavioral, and deeply human.
1. Notification and Communication
Notification is not only about whether an alert is sent.
It is about whether the alert is received, noticed, understood, trusted, and actionable.
A loud alarm may alert one person and overwhelm another. A verbal announcement may be clear to some people and inaccessible to others. A text alert may help, but only if the instruction is specific, plain, and connected to the environment people are actually in.
Good emergency communication should not depend on one channel. It should be multimodal, clear, consistent, and easy to act on under stress.
2. Evacuation, Navigation, and Wayfinding
Evacuation is not only about whether an exit route exists.
It is about whether people can find it, understand it, access it, and move through it under pressure.
Wayfinding that feels adequate on a normal day can break down during an emergency. Crowds shift sightlines. Noise affects attention. Stress affects memory and decision-making. A sign that is technically present may not be useful if it is not visible, legible, or connected to a clear sequence of movement.
A plan that says “exit through Stair B” assumes people know where Stair B is, can reach it, can tolerate the crowd around it, and can make that decision quickly.
Neuroinclusive emergency planning asks whether those assumptions are true.
3. Sheltering in Place
Sheltering in place is often described as staying where you are. But in practice, it is a sensory and social experience.
What does it feel like to wait in a crowded room, lobby, corridor, stairwell, or assembly area while alarms are sounding and people are talking over one another?
Is there a place of lower stimulation?
Is there clear information about what is happening?
Can people sit?
Can they separate from the crowd if needed?
Can they understand whether they are safe, what is expected, and what will happen next?
For some people, the shelter environment itself can become a source of distress. That does not mean sheltering is wrong. It means sheltering needs to be designed with human variability in mind.
4. Operations and First Response
Operations and first response are not only about command and control. They are about human interaction under pressure.
Staff and responders are often expected to guide people quickly in uncertain conditions. But if protocols do not account for sensory overload, processing delays, communication differences, trauma responses, or behavioral misinterpretation, emergency response can unintentionally create additional conflict or harm.
A person who cannot move immediately may need support, not pressure.
A person who is overwhelmed may need space, not escalation.
A person who is not responding verbally may still understand, or may need another form of communication.
Neuroinclusive emergency planning helps staff and responders distinguish distress from defiance and support from control.
Why Architects Have a Unique Role
Architects have a unique role because they influence the conditions that shape emergency behavior before an emergency ever happens.
They shape spatial legibility. They shape wayfinding. They shape acoustics, lighting, thresholds, circulation, exits, gathering areas, refuge spaces, sightlines, materials, signage, and the hierarchy of information.
They influence how people understand a building, how they move through it, where they pause, what they notice, and how stress is either reduced or intensified.
When architects engage with emergency planning, the conversation changes from procedure to experience.
That shift is powerful.
It moves the question from “Does the building have a plan?” to “Can people actually use the plan under stress?”
It moves the question from “Are instructions posted?” to “Can people understand and act on them when overwhelmed?”
It moves the question from “Is there an exit route?” to “Is the route legible, reachable, and manageable for different bodies and minds under pressure?”
Designing for neuroinclusion is not about adding special accommodations at the end. It is about asking better questions at the beginning.
Designing for Stress Often Makes Systems Better for Everyone
One of the most important lessons of inclusive design is that designing for people with specific needs often improves the experience for many more people.
Plain language helps everyone.
Multimodal communication helps everyone.
Clear wayfinding helps everyone.
Lower-stimulation waiting areas help everyone.
Staff trained to recognize distress without escalating it help everyone.
Better lighting, better acoustics, better thresholds, better circulation, and better communication hierarchy help everyone.
This is not about designing for a small edge case. It is about recognizing that stress changes all of us.
The same person who easily navigates a building on a normal day may struggle during an emergency. The same person who understands instructions in a meeting may miss them when alarms are sounding. The same person who moves confidently through a lobby may freeze when the crowd changes direction.
Neuroinclusive design gives us a more honest model of human behavior.
Where Access Built’s AIDE Work Fits In
At Access Built, we are exploring this through our emerging AIDE work.
AIDE is being developed to help organizations stress-test emergency plans before a real emergency exposes the failure.
The goal is not to replace emergency managers, architects, facility teams, operators, or first responders. The goal is to help them see where a plan may break down for real people under real conditions.
AIDE looks at the relationship between emergency plans, built environments, communication systems, staff protocols, and human behavior. It asks where friction may occur across notification, evacuation, sheltering, and response. It helps identify assumptions that may be invisible in a traditional plan review but become very visible under stress.
At this stage, we are being careful not to overstate what the work can do. Emergency readiness is complex. Buildings are different. People are different. Scenarios are different.
But the direction is clear.
Organizations need better ways to test how emergency systems perform before people are placed at risk.
They need ways to see where communication may fail, where movement may break down, where sheltering may become overwhelming, and where staff interactions may unintentionally escalate distress.
That is the opportunity.
Before the Emergency
The time to ask these questions is before the emergency.
Before the alarm sounds.
Before people are confused.
Before a crowd forms.
Before staff have to make fast decisions.
Before a person in distress is misunderstood.
Before a plan that looked complete on paper is tested by real life.
The upcoming AIANY Social Science and Architecture event is meaningful because it brings architecture, design psychology, lived experience, and emergency planning into the same room. That combination is powerful because no single discipline can solve this alone.
Emergency planning needs operations.
It needs compliance.
It needs facilities expertise.
It needs trained responders.
It also needs design.
Because the measure of an emergency plan is not whether it looks complete in a document. It is whether people can receive information, understand what to do, move safely, wait safely, regulate stress, and interact safely with the people trying to help them.
That is the work ahead.
And it is design work.
Key Takeaways
Neuroinclusive emergency planning asks whether emergency systems work for real people under sensory, cognitive, and emotional stress.
The built environment shapes how people receive information, navigate space, shelter, regulate stress, and interact with staff or responders.
Emergency conditions are a crash test for emergency plans because they reveal whether procedures actually perform under pressure.
Architects play a critical role in emergency readiness because they influence spatial legibility, wayfinding, acoustics, lighting, thresholds, circulation, refuge areas, and communication hierarchy.
Designing for neuroinclusion often creates clearer, calmer, and safer systems for everyone.
FAQ
What is neuroinclusive emergency planning?
Neuroinclusive emergency planning is an approach to emergency readiness that considers how neurodivergent people and people with sensory, cognitive, or communication needs may experience alerts, evacuation routes, sheltering, staff instructions, and first response interactions under stress.
Why is emergency planning a design issue?
Emergency planning is a design issue because buildings shape how people receive information, understand instructions, move through space, wait safely, and interact with staff or responders. A plan may exist on paper, but the built environment strongly influences whether people can actually use it.
How does neuroinclusive design improve emergency response?
Neuroinclusive design improves emergency response by reducing confusion, sensory overload, communication barriers, and unnecessary escalation. It encourages clearer alerts, better wayfinding, calmer sheltering conditions, and staff protocols that recognize human behavior under stress.
Why do emergency plans need to be stress-tested?
Emergency plans need to be stress-tested because a plan that appears complete in a document may not work for real people during an actual emergency. Stress can affect attention, memory, movement, communication, and decision-making. Stress-testing helps identify where plans may break down before a real emergency occurs.
What is AIDE?
AIDE is Access Built’s emerging work to help organizations stress-test emergency plans before a real emergency exposes the failure. It looks at the relationship between emergency plans, buildings, communications, staff protocols, and human behavior to identify where friction may occur for people under stress.
Want to stress-test your emergency plan through a neuroinclusive design lens? Contact Access Built.